Key Takeaways
- Arteriosclerosis is a broad term for stiff, thickened artery walls.
- Atherosclerosis is one type of arteriosclerosis that forms plaque.
- Plaque can narrow blood flow and raise heart attack risk.
- Stiff arteries can strain the heart even without major plaque.
- The two terms overlap, but they do not mean the same thing.
Basic Meaning
People often use these two words as if they mean the same thing. That mix-up is common, but the terms describe different changes in the arteries.
Arteriosclerosis is the broad term. It means the arteries become thicker, less elastic, and more stiff over time. That change can happen with age, high blood pressure, diabetes, kidney disease, and other long-term stress on the artery wall (Mitchell and Powell, 2020; Park and Avolio, 2023).
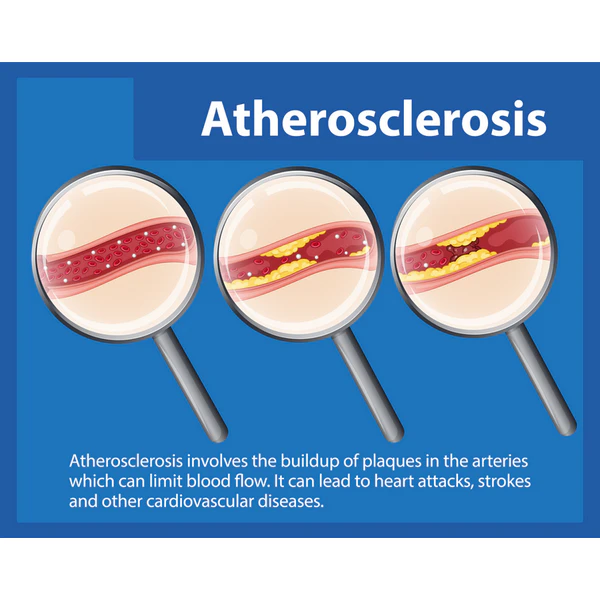
Atherosclerosis is one type of arteriosclerosis. In this form, plaque builds inside the artery wall. Plaque is made from fat, cholesterol, calcium, cell waste, and inflammatory cells. Over time, that buildup can make the opening of the artery more narrow and less stable (Dos Santos et al., 2021; Libby, 2021).
The simplest way to tell them apart is Arteriosclerosis means artery hardening or stiffening in a broad sense. Atherosclerosis means plaque disease inside the arteries.
One Is Broader
Doctors and researchers use arteriosclerosis as an umbrella term. It can include stiffness of large arteries, disease of small arteries, and calcium changes in the vessel wall. Atherosclerosis sits under that umbrella as one specific pattern of disease (Dos Santos et al., 2021).
A person may have arteriosclerosis without having heavy plaque buildup. The reverse is also true in a practical sense, because plaque disease often comes with stiffening as it grows.
What Happens In The Artery
Arteries are meant to stretch with each heartbeat. Healthy artery walls help move blood forward with less strain on the heart. With arteriosclerosis, the wall becomes less springy. Structural parts of the wall change over time. The vessel may hold more stiff material and lose some of the soft, elastic parts that help it expand and recoil. This process can raise pulse pressure and increase the force the heart must work against (Mitchell and Powell, 2020; Vlachopoulos et al., 2010).
With atherosclerosis, the inner layer of the artery becomes injured or disturbed. Lipids and immune cells collect there. The area becomes inflamed, then forms plaque. Some plaques stay stable for years. Others may rupture and trigger a clot, which can suddenly block blood flow to the heart or brain (Gimbrone and García-Cardeña, 2016; Davignon and Ganz, 2004).
Stiffness Vs Plaque
This is the key difference:
- Arteriosclerosis mainly describes loss of flexibility in the artery wall.
- Atherosclerosis mainly describes plaque buildup within the artery wall.
In real life, these changes often appear together. Research has shown links between arterial stiffness and later plaque or heart disease, but they are still not identical conditions (Palombo et al., 2016; Oberoi et al., 2013).
Why The Difference Matters
Arteriosclerosis can increase the speed of the pulse wave moving through the arteries. That change can raise blood pressure load, stress the heart, and damage delicate blood vessels in organs such as the brain and kidneys. Aortic pulse wave velocity, a common measure of arterial stiffness, has been linked with future cardiovascular events and death in pooled studies (Ben-Shlomo et al., 2014; Vlachopoulos et al., 2010).
Atherosclerosis can reduce blood flow or suddenly block it. When plaque grows in the coronary arteries, it can lead to chest pain or heart attack. When it affects the carotid arteries, it can raise stroke risk. When it affects leg arteries, it can cause walking pain or poor wound healing (Libby, 2021).
How They Are Measured
Arterial stiffness is often assessed with pulse wave velocity or other measures of how pressure waves move through the arteries. Faster wave speed usually means a stiffer vessel wall (Park and Avolio, 2023; Ben-Shlomo et al., 2014).
Atherosclerosis is often assessed with imaging that looks for plaque or thickening in the artery wall. Carotid ultrasound may measure intima-media thickness and may also detect plaque. Coronary calcium scans and CT angiography can also show signs of plaque burden in some people (van den Oord et al., 2013; Willeit et al., 2020).
These tests do not answer the same question. One test asks how stiff the artery is. Another asks whether plaque is present, growing, or likely to narrow flow.
Symptoms And Risk
Neither condition always causes symptoms early on. That is one reason the terms cause confusion. A person may have years of silent artery changes before warning signs show up.
Arteriosclerosis by itself may not cause a clear symptom at first. Instead, it may show up through rising blood pressure, widening pulse pressure, or signs of strain on the heart. In some studies, systemic arterial stiffness has been linked with heart remodeling even when plaque burden did not show the same pattern (Weir-McCall et al., 2018).
Atherosclerosis may also stay silent for years. Symptoms often depend on where the plaque is found. Narrowing in heart arteries may cause chest pressure. Disease in the brain circulation may cause stroke or a transient neurologic event. Leg artery plaque may cause pain with walking that eases with rest (Libby, 2021).
Shared Risk Factors
The two conditions share many drivers. These include aging, smoking, high blood pressure, diabetes, kidney disease, and long-term metabolic stress.
Some cohort studies have shown that higher arterial stiffness is linked with future plaque formation or greater subclinical plaque burden, which shows how these processes can move together over time (Yang et al., 2018; Li et al., 2022). Still, the overlap should not erase the difference. One process focuses on wall mechanics. The other focuses on plaque biology.
Simple Clinical Picture
For general readers, this framework is useful and easy to remember. Arteriosclerosis is the big category. It describes arteries that have become more stiff, thick, or less flexible.
Atherosclerosis is the plaque subtype. It describes fatty, inflamed, and often calcified buildup inside artery walls.
You can have both at the same time. In fact, many older adults with vascular disease do. Yet the terms are not perfect substitutes, and careful writing should keep them separate (Dos Santos et al., 2021; Park and Avolio, 2023).
Way To Remember
A simple memory aid can help. Arteriosclerosis refers to hardening and stiffening of arteries in general. Atherosclerosis refers to a plaque process inside the arteries. That one distinction clears up most of the confusion around these closely related words.
Before changing your diet, supplements, or health routine, talk with a licensed healthcare professional. For any health concerns or questions about a medical condition, get guidance from a physician or another appropriately trained clinician.
FAQs
Is atherosclerosis a type of arteriosclerosis?
Yes. Atherosclerosis is one specific type of arteriosclerosis. It involves plaque buildup inside the artery wall, while arteriosclerosis is the broader term for artery thickening and stiffening.
Can someone have arteriosclerosis without atherosclerosis?
Yes. Arteries can become stiff with age, pressure load, or other disease without large plaque deposits being present. That is one reason the two terms should not be used as exact matches.
Which one causes heart attacks more directly?
Atherosclerosis is more directly tied to heart attacks because plaque can narrow a coronary artery or rupture and trigger a clot. Arterial stiffness still matters because it increases strain on the heart and blood vessels.
Do both conditions raise stroke risk?
Yes. Atherosclerosis can raise stroke risk through plaque in arteries that feed the brain. Arteriosclerosis can also harm blood vessel health and contribute to vascular risk over time.
How do doctors tell them apart?
Doctors often use different tests. Arterial stiffness can be measured with pulse wave velocity, while plaque disease is often assessed with ultrasound, calcium scoring, or CT imaging.
Research
Willeit, P. et al. (2020) ‘Carotid Intima-Media Thickness Progression as Surrogate Marker for Cardiovascular Risk: Meta-Analysis of 119 Clinical Trials Involving 100 667 Patients’, Circulation, 142(7), pp. 621–642. Available at: https://pubmed.ncbi.nlm.nih.gov/32546049/
van den Oord, S.C.H. et al. (2013) ‘Carotid intima-media thickness for cardiovascular risk assessment: systematic review and meta-analysis’, Atherosclerosis, 228(1), pp. 1–11. Available at: https://pubmed.ncbi.nlm.nih.gov/23395523/
Ben-Shlomo, Y. et al. (2014) ‘Aortic pulse wave velocity improves cardiovascular event prediction: an individual participant meta-analysis of prospective observational data from 17,635 subjects’, Journal of the American College of Cardiology, 63(7), pp. 636–646. Available at: https://pubmed.ncbi.nlm.nih.gov/24239664/
Vlachopoulos, C. et al. (2010) ‘Prediction of cardiovascular events and all-cause mortality with arterial stiffness: a systematic review and meta-analysis’, Journal of the American College of Cardiology, 55(13), pp. 1318–1327. Available at: https://pubmed.ncbi.nlm.nih.gov/20338492/
Dos Santos, V.P. et al. (2021) ‘Arteriosclerosis, atherosclerosis, arteriolosclerosis, and Monckeberg medial calcific sclerosis: what is the difference?’, Journal of Vascular Brasileiro, 20, e20200211. Available at: https://pubmed.ncbi.nlm.nih.gov/34290756/
Park, J.B. and Avolio, A. (2023) ‘Arteriosclerosis and Atherosclerosis Assessment in Clinical Practice: Methods and Significance’, Pulse (Basel), 11(1), pp. 1–8. Available at: https://pubmed.ncbi.nlm.nih.gov/37404379/
Libby, P. (2021) ‘The changing landscape of atherosclerosis’, Nature, 592(7855), pp. 524–533. Available at: https://pubmed.ncbi.nlm.nih.gov/33883728/
Gimbrone, M.A. Jr and García-Cardeña, G. (2016) ‘Endothelial Cell Dysfunction and the Pathobiology of Atherosclerosis’, Circulation Research, 118(4), pp. 620–636. Available at: https://pubmed.ncbi.nlm.nih.gov/26892962/
Davignon, J. and Ganz, P. (2004) ‘Role of endothelial dysfunction in atherosclerosis’, Circulation, 109(23 Suppl 1), pp. III27–III32. Available at: https://pubmed.ncbi.nlm.nih.gov/15198963/
Palombo, C. et al. (2016) ‘Arterial stiffness, atherosclerosis and cardiovascular risk: Pathophysiologic mechanisms and emerging clinical indications’, Vascular Pharmacology, 77, pp. 1–7. Available at: https://pubmed.ncbi.nlm.nih.gov/26643779/
Oberoi, S. et al. (2013) ‘Progression of arterial stiffness and coronary atherosclerosis: longitudinal evaluation by cardiac CT’, American Journal of Roentgenology, 200(4), pp. 798–804. Available at: https://pubmed.ncbi.nlm.nih.gov/23521451/
Weir-McCall, J.R. et al. (2018) ‘Systemic arteriosclerosis is associated with left ventricular remodeling but not atherosclerosis: a TASCFORCE study’, Journal of Cardiovascular Magnetic Resonance, 20(1), 7. Available at: https://pubmed.ncbi.nlm.nih.gov/29382349/
Yang, Y. et al. (2018) ‘Brachial-Ankle Pulse Wave Velocity is Associated with the Risk of New Carotid Plaque Formation: Data from a Chinese Community-based Cohort’, Scientific Reports, 8(1), 7037. Available at: https://pubmed.ncbi.nlm.nih.gov/29728607/
Li, W. et al. (2022) ‘Evaluation of Carotid Artery Atherosclerosis and Arterial Stiffness in Cardiovascular Disease Risk: An Ongoing Prospective Study From the Kailuan Cohort’, Frontiers in Cardiovascular Medicine, 9, 812652. Available at: https://pubmed.ncbi.nlm.nih.gov/35586658/
Lorenz, M.W. et al. (2007) ‘Prediction of clinical cardiovascular events with carotid intima-media thickness: a systematic review and meta-analysis’, Circulation, 115(4), pp. 459–467. Available at: https://pubmed.ncbi.nlm.nih.gov/17242284/
Weber, T. et al. (2004) ‘Arterial stiffness, wave reflections, and the risk of coronary artery disease’, Circulation, 109(2), pp. 184–189. Available at: https://pubmed.ncbi.nlm.nih.gov/14662706/
Cederqvist, J. et al. (2023) ‘Arterial stiffness and subclinical atherosclerosis in the coronary arteries at different stages of dysglycaemia’, Diabetic Medicine, 40(7), e15102. Available at: https://pubmed.ncbi.nlm.nih.gov/37004152/
Del Brutto, O.H. et al. (2020) ‘The association between aortic arterial stiffness, carotid intima-media thickness and carotid plaques in community-dwelling older adults: A population-based study’, Vascular, 28(4), pp. 405–412. Available at: https://pubmed.ncbi.nlm.nih.gov/32228175/
Bae, J.S. et al. (2013) ‘The impact of serum uric acid level on arterial stiffness and carotid atherosclerosis: the Korean Multi-Rural Communities Cohort study’, Atherosclerosis, 231(1), pp. 145–151. Available at: https://pubmed.ncbi.nlm.nih.gov/24125426/
Mitchell, G.F. and Powell, J.T. (2020) ‘Arteriosclerosis: A Primer for “In Focus” Reviews on Arterial Stiffness’, Arteriosclerosis, Thrombosis, and Vascular Biology, 40(5), pp. 1025–1027. Available at: https://pubmed.ncbi.nlm.nih.gov/32320295/