Key Takeaways
- Keto can help some adults lose body fat over several months with steady food choices.
- Blood sugar often drops when carbs stay very low, especially in type 2 diabetes.
- Seizure control remains the strongest medical use, especially in drug resistant epilepsy care.
- Long term results depend on food quality, enough support and a plan you can keep.
- Whole animal foods, natural fats and fewer carbs make keto easier to sustain.
Keto Basics
Fuel Shift
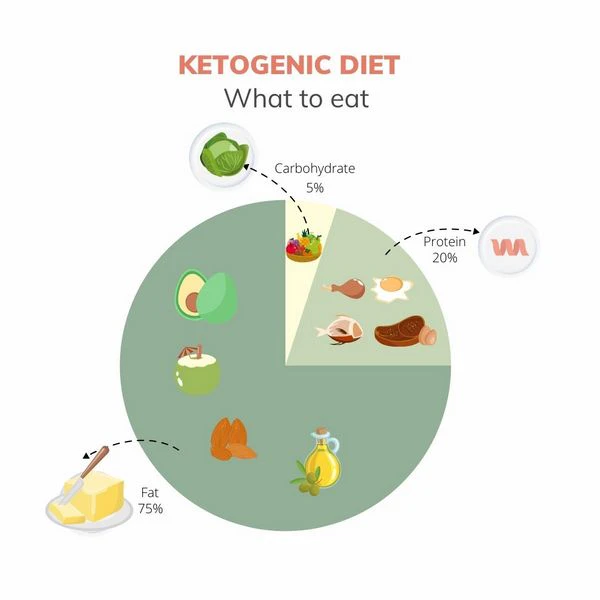
A ketogenic diet keeps carbs very low so your body makes more ketones. Ketones come from fat. Your liver makes them when sugar from food drops low enough.
Many people use keto for fat loss because it removes the main foods that keep hunger high and blood sugar moving up and down all day.
Keto usually means meat, eggs, seafood, butter, ghee, tallow and other natural fats. Many people also use small amounts of lower carb plants if they digest them well.
The stronger version removes grains, sugar, seed oils, fortified foods and most packaged foods.
Food quality changes the result because keto made from processed bars and seed oil snacks does not act like keto made from real food.
Lower Insulin
Carbs raise blood sugar more than fat or protein. Your body responds by releasing insulin. Insulin helps move sugar out of the blood.
Lower carb intake often lowers daily insulin demand. Many adults feel steadier energy when blood sugar swings become smaller.
Lower insulin also changes fuel use. Stored fat becomes easier to release when insulin stays lower for longer parts of the day.
The body still needs enough food and enough protein, because forced hunger can backfire. Keto works best when you eat enough real food and let lower hunger happen naturally.
A large review of trials in adults with type 2 diabetes found that very low carbohydrate diets may lower HbA1c and triglycerides, though long term advantage over other diets was less certain across all trials (1).
The useful point is still clear. Carb restriction often gives fast blood sugar changes, especially in people who start with high blood sugar.
Food Quality
Keto gives the best return when the base food is simple. Grass fed ruminant meat, organs, pasture raised eggs, wild seafood, butter, ghee and tallow give protein, fat and minerals without a carb load.
These foods also make the diet easier because they satisfy hunger without needing snacks every few hours.
Poor keto food choices can make the diet harder. Packaged keto desserts, seed oil sauces and sweetened products can keep cravings alive.
Many people do better when keto stays close to normal food. Eat meals, stop snacking and make the diet boring enough that your appetite can calm down.
Fat Loss Benefits
Several Month Results
Keto can help fat loss because it removes sugar, grains and many snack foods at the same time. Many adults also eat fewer calories without tracking because protein and fat are more filling.
A review of randomized trials found that very low carbohydrate ketogenic diets led to greater long term weight loss than low fat diets, though the average difference was modest (2).
Another meta analysis in overweight adults with type 2 diabetes found better body weight, waist size, HbA1c, triglycerides and HDL results with ketogenic diets across eight randomized trials (3).
The benefit looks strongest in the first several months. Many diets show weaker results later because people drift back toward old food.
Keto can also make hunger easier to manage. When protein stays high enough and carbs stay low, many people stop needing constant snacks. Blood sugar swings often become smaller.
Food thoughts can drop because the diet removes the sweet foods that train the brain to keep asking for more.
Body Composition
Fat loss works better when muscle is protected. Keto should not mean tiny meals and low protein.
You need enough meat, eggs, seafood and other protein rich food to keep lean tissue strong. Strength training adds another signal to keep muscle while fat is lost.
A small controlled feeding study found that a ketogenic diet changed fuel use toward more fat oxidation, though the measured fat loss advantage was limited in that short lab setting (4).
Lab studies can control food tightly. Real life keto often works through lower hunger, simpler food choices and fewer trigger foods.
Scale weight can drop quickly at first because stored carbohydrate holds water. Early weight loss is not all fat.
After that first drop, waist size, strength and steady hunger tell you more than the scale alone. Keto is more useful when it becomes a repeatable food routine instead of a short challenge.
Protein And Fat Drive Satiety
Animal based meals are harder to overeat when protein and fat replace sugar and snack foods.
Blood Sugar Benefits
Type 2 Diabetes
Keto has some of its clearest everyday value in type 2 diabetes because carbs directly raise blood sugar.
A 12 month randomized trial found that adults assigned to a very low carbohydrate ketogenic diet had greater HbA1c reduction, greater weight loss and larger reductions in diabetes drug use than those assigned to a moderate carbohydrate reduced calorie low fat diet (5).
A 24 week trial in adults with obesity and type 2 diabetes compared a low carbohydrate ketogenic diet with a low glycemic reduced calorie diet.
Both groups improved, while the ketogenic group had stronger improvements in glycemic control and more medication reduction (6).
Those results make sense because carbohydrate is the main food driver of post food glucose.
Blood sugar can fall quickly on keto. Anyone using glucose lowering drugs needs proper medical oversight because the same drug dose can become too strong after carbs drop.
The diet changes the demand placed on the body. Drugs can also change the risk picture, so supervision is sensible when blood sugar is already being treated.
Hunger & Cravings
Keto often reduces cravings because it removes the foods that create the biggest reward loop. Sugar, flour and sweet drinks train repeat hunger.
A meal based on meat, eggs and natural fat usually gives a slower and steadier signal to the brain.
Stable blood sugar also helps mood and focus for some people. Large swings can feel like sudden hunger, shakes, sleepiness or irritability.
Keto cannot fix every cause of low energy, but fewer blood sugar swings can make daily food control easier.
Use vs Avoid
| Use | Avoid |
|---|---|
| Ruminant meat | Seed oils |
| Eggs | Sugar drinks |
| Seafood | Packaged snacks |
| Animal fats | Fortified grains |
Medical Uses
Seizure Control
Seizure control remains the strongest established medical use of keto. The diet was used for epilepsy long before it became popular for weight loss.
A Cochrane review found that ketogenic diets improved seizure freedom and seizure reduction in children with drug resistant epilepsy, while the certainty of evidence ranged from low to very low because blinding diet trials is hard (7).
The epilepsy evidence is important because it shows that keto is not only a weight loss idea. It changes brain fuel use, blood chemistry and energy handling.
Children with hard to control seizures may need a medical keto team because the diet has to be measured and monitored more tightly than casual adult keto.
Adults with seizures have less trial evidence than children. Reviews still describe keto as a serious option in specialist care for some cases.
The strength of evidence varies by age, seizure type and diet version, so medical use belongs under trained supervision.
Brain Energy
Ketones can fuel the brain when glucose intake is low. The brain still uses some glucose, but it can use ketones for a large share of energy during ketosis.
Many people report clearer thinking on keto, though personal reports are stronger than hard proof for general brain performance.
Keto also changes appetite signals. Lower insulin, steadier blood sugar and higher ketones may all help reduce hunger.
The exact mix differs by person. The simple result is what most people notice first. They can go longer between meals without feeling driven by cravings.
Animal Based Check
Long Term Success
Consistency
Long term results depend on whether you can keep the diet in normal life. Keto is easier when you use real meals instead of special products.
Meat, eggs, seafood and natural fats keep choices clear. You do not need complicated recipes to get results.
A review of recent trials in type 2 diabetes found that keto may improve lipid markers, while extra benefits for glycemic control or weight loss over other diets were less clear over longer follow up (8).
Support helps because the first month can feel different. Salt and fluid needs can change as insulin falls.
Some people feel tired during the shift. Enough food, enough protein and enough minerals make the change easier.
Sensible Tracking
Good tracking does not need to become obsessive. Waist size, fasting glucose, post food glucose, energy, sleep and hunger give useful feedback.
Blood ketones can help at first, especially when you are learning which foods keep you in ketosis.
Keto should feel steady after the adaptation stage. Constant fatigue, poor sleep or ongoing digestive trouble means something needs to change.
Many problems come from eating too little, using poor quality fats or relying on processed keto foods. Simple meals fix many of those mistakes.
Best Food Base
The strongest keto base is whole food and high in natural fat. Grass fed beef, lamb, bison, liver, eggs, sardines, salmon, butter, ghee and tallow are useful staples.
Small amounts of cucumber, lettuce or cabbage can be used if tolerated.
Seed oils, fortified grain products and sweetened keto snacks weaken the diet. They keep the old food system inside a new label. Better keto is normal food with carbs removed. That style gives your body protein, minerals and fat without the blood sugar load.
For any health concerns or questions about a medical condition, get guidance from a physician or another appropriately trained clinician. Before changing your diet, supplements or health routine, talk with a licensed healthcare professional.
Suggested Posts


Research
Parry Strong, A. et al. 2022. Very low carbohydrate ketogenic diets in type 2 diabetes: A systematic review and meta analysis of randomized controlled trials. Diabetes, Obesity and Metabolism. DOI: 10.1111/dom.14837. PMID: 36064937.
Bueno, N.B. et al. 2013. Very low carbohydrate ketogenic diet v. low fat diet for long term weight loss: a meta analysis of randomised controlled trials. British Journal of Nutrition. DOI: 10.1017/S0007114513000548. PMID: 23651522.
Zhou, C. et al. 2022. Ketogenic Diet Benefits to Weight Loss, Glycemic Control, and Lipid Profiles in Overweight Patients with Type 2 Diabetes Mellitus: A Meta Analysis of Randomized Controlled Trails. International Journal of Environmental Research and Public Health. DOI: 10.3390/ijerph191610429. PMID: 36012064.
Hall, K.D. et al. 2016. Energy expenditure and body composition changes after an isocaloric ketogenic diet in overweight and obese men. The American Journal of Clinical Nutrition. DOI: 10.3945/ajcn.116.133561. PMID: 27385608.
Saslow, L.R. et al. 2017. Twelve month outcomes of a randomized trial of a moderate carbohydrate versus very low carbohydrate diet in overweight adults with type 2 diabetes mellitus or prediabetes. Nutrition & Diabetes. DOI: 10.1038/s41387-017-0006-9. PMID: 29269731.
Westman, E.C. et al. 2008. The effect of a low carbohydrate, ketogenic diet versus a low glycemic index diet on glycemic control in type 2 diabetes mellitus. Nutrition & Metabolism. DOI: 10.1186/1743-7075-5-36. PMID: 19099589.
Martin McGill, K.J. et al. 2020. Ketogenic diets for drug resistant epilepsy. Cochrane Database of Systematic Reviews. DOI: 10.1002/14651858.CD001903.pub5. PMID: 32588435.
Choy, K.Y.C. et al. 2023. The ketogenic diet for type 2 diabetes mellitus: A systematic review and meta analysis of recent studies. Diabetes & Metabolic Syndrome. DOI: 10.1016/j.dsx.2023.102873. PMID: 38006799.
Ghasemi, P. et al. 2024. Impact of very low carbohydrate ketogenic diets on cardiovascular risk factors among patients with type 2 diabetes: GRADE assessed systematic review and meta analysis of randomized controlled trials. Nutrition, Metabolism and Cardiovascular Diseases. PMID: 39030553.
Luo, W. et al. 2022. Low carbohydrate ketogenic diets reduce cardiovascular risk factor levels in obese or overweight patients: A meta analysis of randomized controlled trials. Frontiers in Nutrition. DOI: 10.3389/fnut.2022.1092031. PMID: 36583214.
Tinguely, D. et al. 2021. Efficacy of ketogenic diets on type 2 diabetes: a systematic review. Current Diabetes Reports. DOI: 10.1007/s11892-021-01399-z. PMID: 34448957.
Yancy, W.S. Jr. et al. 2004. A low carbohydrate, ketogenic diet versus a low fat diet to treat obesity and hyperlipidemia: a randomized, controlled trial. Annals of Internal Medicine. DOI: 10.7326/0003-4819-140-10-200405180-00006. PMID: 15148063.
Yancy, W.S. Jr. et al. 2005. A low carbohydrate, ketogenic diet to treat type 2 diabetes. Nutrition & Metabolism. DOI: 10.1186/1743-7075-2-34. PMID: 16318637.
Saslow, L.R. et al. 2017. An online intervention comparing a very low carbohydrate ketogenic diet and lifestyle recommendations versus a plate method diet in overweight individuals with type 2 diabetes: a randomized controlled trial. Journal of Medical Internet Research. DOI: 10.2196/jmir.5806. PMID: 28193599.