Key Takeaways
- Calcium and phosphate stay in range through bone, gut, kidneys, and hormones.
- The kidneys remove extra phosphate and help keep blood calcium steady.
- Low vitamin D or kidney disease can upset this balance fast.
- Blood tests for calcium, phosphate, and parathyroid hormone can show problems.
- Food, kidney health, and the right treatment plan guide safe correction.
Why Balance Works
Blood Needs Steady Levels
Calcium and phosphate must stay in a narrow range in your blood. Your nerves, muscles, heart, and cells depend on that steady range every hour of the day (Shaker and Deftos, 2023; Yu and Sharma, 2023).
Your body does not leave this job to chance. It shifts these minerals between the gut, blood, bone, and urine all day long.
That is why a normal blood test can reflect a very active control system, not a still one (Shaker and Deftos, 2023).
Bones Hold The Reserve
Most of the body’s calcium and phosphate sit in bone. Bone is not a dead storehouse. It is living tissue that is always breaking down a bit and building back up again.
That gives the body a reserve to draw on when blood levels drift. When blood calcium falls, the body can move calcium out of bone to keep the heart and nerves working.
It helps in the short term, though it can weaken bone when the problem goes on for too long (Shaker and Deftos, 2023; NIDDK, 2025a).
Who Keeps Control
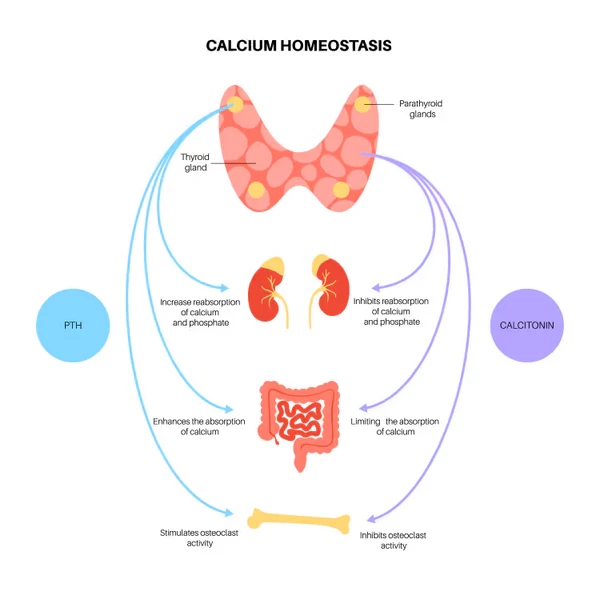
Hormones Direct Traffic
Three main signals help direct calcium balance. They are parathyroid hormone, active vitamin D, and calcitonin.
A fourth signal called FGF23 has a strong effect on phosphate control, most of all through the kidneys (Yu and Sharma, 2023; Shaker and Deftos, 2023).
Parathyroid hormone rises when blood calcium drops. It tells the kidneys to save more calcium, tells bone to release some calcium, and helps the body make more active vitamin D.
Active vitamin D then helps the gut absorb more calcium and phosphate from food (Yu and Sharma, 2023).
FGF23 works more on phosphate. It helps the body get rid of extra phosphate in urine and also affects vitamin D activity.
This keeps phosphate from climbing too high after intake from food or release from bone (Shaker and Deftos, 2023; Shah and Mathew, 2024).
The Kidneys Set The Pace
The kidneys are central to this balance. They remove extra phosphate, fine tune calcium handling, and activate vitamin D into a form the body can use well.
When kidney function falls, phosphate often starts to build up in the blood. The body then raises hormone signals to defend blood calcium.
Over time, that strain can pull calcium from bone and raise the risk of weak bones, blood vessel calcification, and heart trouble (NIDDK, 2025a; Shah and Mathew, 2024).
Calcium Supplements Need Caution
Calcium supplements are not the same thing as calcium inside food.
When Balance Shifts
Low Calcium
Low blood calcium can happen for many reasons. Low vitamin D, low magnesium, poor absorption, some hormone problems, pancreatitis, and kidney disease are common causes.
In some cases, a high phosphate level also drives calcium down.
Symptoms can include tingling around the mouth, muscle cramps, hand or foot spasms, and in more severe cases seizures or heart rhythm problems.
Mild cases may cause no clear symptoms at first, which is why lab tests often find the problem before a person feels very ill (Yu and Sharma, 2023).
High Phosphate
High phosphate is most common in chronic kidney disease because the kidneys cannot clear the extra load well.
When phosphate stays high, it can lower blood calcium and push parathyroid hormone up. That can harm bone over time.
In people with chronic kidney disease, high phosphate is linked with thin weak bones, itching, bone pain, and calcium deposits in blood vessels and soft tissues.
Those deposits can raise the risk of heart and blood vessel disease (NIDDK, 2025b; NIDDK, 2025a).
Low Phosphate
Low phosphate gets less attention, yet it can also be serious. Severe loss can weaken muscles, reduce energy, and in some cases affect breathing, heart function, or bone strength.
This can happen with poor intake, alcohol misuse, gut problems, some medicines, severe illness, or a fast shift of phosphate into cells during recovery from starvation or diabetic crisis.
The cause must guide the fix because the wrong treatment can worsen the problem.
Use vs Skip
| Use | Skip |
|---|---|
| Calcium from food | Calcium Supplements |
| Magnesium | Popular advice |
| Vitamin K from food | Ignoring magnesium |
| Full mineral view | Ignoring soft tissue risk |
What Tests Show
Blood Work Gives The Clues
Doctors often check total calcium, albumin, phosphate, kidney function, parathyroid hormone, and vitamin D.
Albumin is checked because part of the calcium in blood is bound to protein. When albumin is low, the total calcium number can look low even when the active calcium is normal.
Ionized calcium is the active form in blood. When the case is complex, ionized calcium can give a clearer picture than total calcium alone. That is useful in very ill patients or when albumin is far from normal.
A single result may not tell the full story. A person can have a normal calcium level while hormone signals are already working hard to hold it there.
That is one reason phosphate, parathyroid hormone, vitamin D, and kidney function are often checked together (Shaker and Deftos, 2023; Shah and Mathew, 2024).
Intake Still Counts
Adults need both minerals, though the daily targets are not the same. The recommended amount for calcium in most adults is about 1,000 milligrams per day, rising to 1,200 milligrams for women age 51 through 70 and all adults over 70.
The recommended amount for phosphorus in adults is 700 milligrams per day (NIH ODS, 2023a; NIH ODS, 2021).
Diet still needs context. Many people get enough phosphate, and some get more than they think because phosphate additives in packaged foods are common.
People with kidney disease often need help from a clinician or kidney dietitian to set a safe limit (NIH ODS, 2023b; NIDDK, 2025b).
Calcium Check
Food & Care
Daily Food Choices
For most healthy adults, balance starts with enough calcium from food and with normal kidney function to clear extra phosphate.
Dairy foods, calcium set tofu, and some fish with soft bones provide calcium. Meat, dairy, beans, nuts, and many packaged foods provide phosphate.
People with healthy kidneys usually handle a normal mixed diet well. Trouble tends to rise when kidney function drops, vitamin D is low, absorption is poor, or a person uses large amounts of supplements without guidance.
For people with chronic kidney disease, phosphate from food additives can be a bigger issue than phosphate from whole foods because it is absorbed well and can push levels up fast.
Reading labels and reviewing a food list with a kidney care team can help lower that load (NIH ODS, 2023b; NIDDK, 2025a).
Treatment Depends On The Cause
A low calcium result is not fixed safely by guessing. The plan depends on why the level changed. One person may need vitamin D support. Another may need magnesium replaced.
A third may need urgent care because the level is dangerously low. High phosphate in chronic kidney disease may call for diet changes, treatment of vitamin D or hormone problems, or other kidney focused care. Blood tests over time guide the plan better than a single number does.
Seek prompt medical care for muscle spasms, seizures, fainting, severe weakness, chest symptoms, or new confusion when a calcium or phosphate problem is suspected.
Before changing your diet, supplements, or health routine, talk with a licensed healthcare professional. For any health concerns or questions about a medical condition, get guidance from a physician or another appropriately trained clinician.
Suggested Posts

Evidence Limits
Research
Shaker, J.L. and Deftos, L. (2023) ‘Calcium and Phosphate Homeostasis’, Endotext. Available at NCBI Bookshelf (Accessed 7 April 2026).
Yu, E. and Sharma, S. (2023) ‘Physiology, Calcium’, StatPearls. Available at NCBI Bookshelf (Accessed 7 April 2026).
NIDDK (2025a) ‘Mineral & Bone Disorder in Chronic Kidney Disease’. Available at National Institute of Diabetes and Digestive and Kidney Diseases (Accessed 7 April 2026).
Shah, A. and Mathew, A.T. (2024) ‘Chronic Kidney Disease Mineral Bone Disorder’, StatPearls. Available at NCBI Bookshelf (Accessed 7 April 2026).
NIDDK (2025b) ‘Healthy Eating for Adults with Chronic Kidney Disease’. Available at National Institute of Diabetes and Digestive and Kidney Diseases (Accessed 7 April 2026).
NIH ODS (2023a) ‘Calcium Fact Sheet for Consumers’. Available at Office of Dietary Supplements (Accessed 7 April 2026).
NIH ODS (2021) ‘Phosphorus Fact Sheet for Consumers’. Available at Office of Dietary Supplements (Accessed 7 April 2026).
NIH ODS (2023b) ‘Phosphorus Health Professional Fact Sheet’. Available at Office of Dietary Supplements (Accessed 7 April 2026).
Bringhurst FR, Demay MB and Kronenberg HM (2018) Hormones and disorders of mineral metabolism. In: Williams Textbook of Endocrinology. Elsevier.
Fukumoto S and Martin TJ (2009) ‘Bone as an endocrine organ’, Trends in Endocrinology & Metabolism.
Martin A, David V and Quarles LD (2012) ‘Regulation and function of the FGF23/Klotho endocrine pathways’, Physiological Reviews.
Razzaque MS (2009) ‘The FGF23–Klotho axis: endocrine regulation of phosphate homeostasis’, Nature Reviews Endocrinology.
Shimada T, Hasegawa H, Yamazaki Y, et al. (2004) ‘FGF-23 is a potent regulator of vitamin D metabolism and phosphate homeostasis’, Journal of Bone and Mineral Research.
Lederer E (2014) ‘Regulation of serum phosphate’, Journal of Physiology.
Blaine J, Chonchol M and Levi M (2015) ‘Renal control of calcium, phosphate, and magnesium homeostasis’, Clinical Journal of the American Society of Nephrology.
Moe SM (2008) ‘Disorders involving calcium, phosphorus, and magnesium’, Primary Care.
Kuro-O M (2010) ‘Klotho’, Pflügers Archiv – European Journal of Physiology.
Quarles LD (2008) ‘Endocrine functions of bone in mineral metabolism regulation’, Journal of Clinical Investigation.
Potts JT (2005) ‘Parathyroid hormone: past and present’, Journal of Endocrinology.
Brown EM (2013) ‘Role of the calcium-sensing receptor in extracellular calcium homeostasis’, Best Practice & Research Clinical Endocrinology & Metabolism.
Christakos S, Dhawan P, Porta A, Mady LJ and Seth T (2011) ‘Vitamin D and intestinal calcium absorption’, Molecular and Cellular Endocrinology.
Dusso AS, Brown AJ and Slatopolsky E (2005) ‘Vitamin D’, American Journal of Physiology-Renal Physiology.
Berndt T and Kumar R (2009) ‘Novel mechanisms in the regulation of phosphorus homeostasis’, Physiology.
Cunningham J, Locatelli F and Rodríguez M (2011) ‘Secondary hyperparathyroidism: pathogenesis, disease progression, and therapeutic options’, Clinical Journal of the American Society of Nephrology.
Hruska KA, Seifert M and Sugatani T (2015) ‘Pathophysiology of the chronic kidney disease–mineral bone disorder’, Current Opinion in Nephrology and Hypertension.